You’ve probably heard the phrase “screen before you treat.” But in the myofunctional therapy world, many clinicians still end up skipping the screen altogether—either because they don’t have a structured tool or because they’re unsure what they’re actually looking for in an orofacial myofunctional disorder screening tool.
That’s exactly what the F.A.S.T. Myo Screening Packet was built to solve.
This post breaks down what this tool is, what each component of this orofacial myofunctional disorder screening tool is designed to assess, what a positive finding actually means, and how to translate those findings into confident, evidence-informed clinical recommendations.
What F.A.S.T. Stands For
F — Function. How is the patient functioning? What is their oral motor pattern like during eating, drinking, speaking, and breathing? Function is the starting point because it tells you what the patient’s daily life actually looks like, not just what you observe during a structured assessment.
A — Airway. Is the patient breathing through their nose or their mouth? Do they have a history of congestion, snoring, sleep disruption, or frequent upper respiratory infections? Airway is the lens through which everything else is interpreted. A mouth breather presents differently than a nasal breather clinically, posturally, and behaviorally.
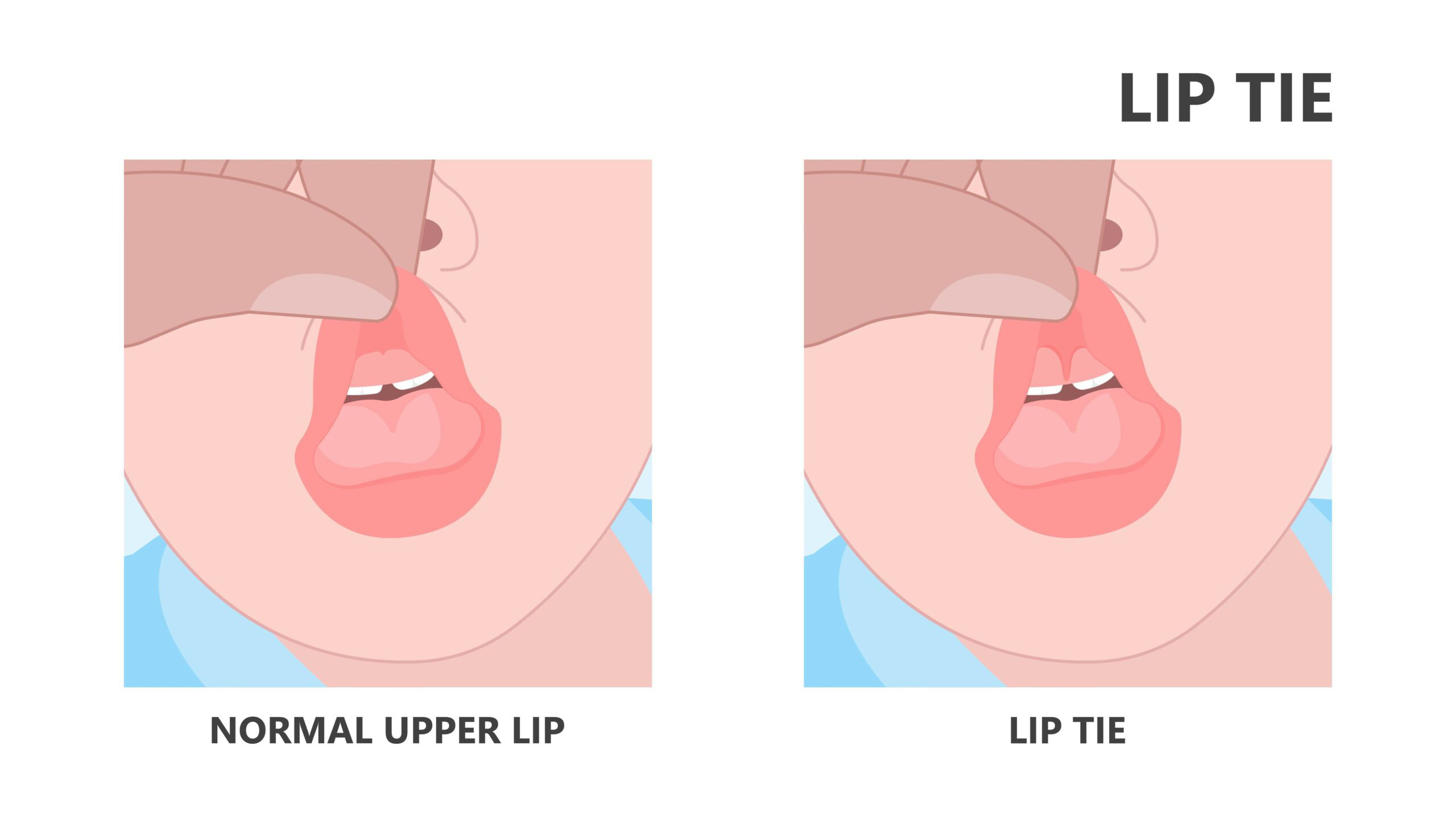
S — Structure. What does the oral structure look like? You’re looking at the frenum (lingual and labial), the palate, the tonsils, the tongue size relative to the oral space, lip tone, and facial morphology. Structure tells you what you’re working with and whether a referral to another provider is warranted before myo begins.
T — Tongue. Where is the tongue at rest? Can the patient elevate to the palate? What does the swallow pattern look like? Is there a tongue thrust? Tongue posture and function are central to virtually every orofacial myofunctional disorder — and the tongue piece alone gives you enormous clinical information.
The Oral Rest Posture Finding Most Clinicians Miss
Of all the things the F.A.S.T. screening looks at, oral rest posture is the one most clinicians overlook or rush through.
Here’s what you’re actually assessing: where does the tongue sit when the patient is doing nothing? Is the tip touching the spot just behind the upper front teeth (the correct resting position)? Or is it sitting on the floor of the mouth, pushing against the lower teeth, or not touching the palate at all?
And equally important: are the lips together at rest? A patient with lips apart at rest is almost always a mouth breather, regardless of what they tell you about their breathing habits.
These two observations, tongue rest posture and lip posture at rest, take about thirty seconds. They tell you an enormous amount about what’s driving the patient’s presentation and what your treatment priorities should be.
What a Positive Screen Means (And What It Doesn’t)
A positive screen means you’ve identified one or more areas that warrant a closer look. It does not mean you have a diagnosis or a treatment plan.
A screen is your permission to look harder. It’s also your clinical justification for having a deeper conversation with the patient and family about what you’re observing.
- If the screen flags airway concerns — significant mouth breathing, a history of sleep disruption, visibly enlarged tonsils — that’s a referral conversation. The patient may need an ENT evaluation before myo therapy is the appropriate next step.
- If the screen flags structural concerns — restricted frenum, narrow palate, significant tonal patterns — that shapes your treatment approach and may indicate an interdisciplinary conversation needs to happen.
- If the screen flags tongue function concerns — low resting posture, tongue thrust swallow, limited elevation — you have the clinical picture you need to move toward a full assessment and treatment plan.
Turning the Screen Into a Clinical Conversation
The F.A.S.T. screen isn’t just a checklist for your own files. It’s a communication tool.
When you can sit with a parent or a patient and say ‘here’s what I observed in each of these four areas, here’s what it means, and here’s what I think the next step is’, that’s what clinical confidence looks like in practice.
It’s also what builds referral relationships. When you screen consistently and communicate your findings clearly to the other providers in the patient’s care circle, the dentist, the pediatrician, the ENT, you position yourself as a specialist who knows what they’re looking at. That’s not something you can fake. And it’s built through both the right tools and the right training.
Download the free F.A.S.T. Myo Screening Packet at fastmyoscreening.com and when you’re ready to build the clinical framework that makes every screen meaningful, explore The Myo Method® and The Myo Membership® at halliebulkin.com