Restricted lingual frenula have real, clinically significant consequences for feeding, speech, and breathing, so the attention is well earned. But here is the part that keeps getting lost: while the whole conversation has centered on the tongue, the lip tie has been getting half the story at best. In clinical practice, that half-told story is exactly how families end up with incomplete assessments, how providers miss functional contributors, and how kids head into frenectomies before anyone has looked at the full picture.
A thorough lip tie functional impact assessment is what closes that gap, and that is what we are going to work through together here. The whole point is to figure out whether the tissue is actually limiting function for the child in front of you, not just whether you can see a frenum when you lift the lip.
Quick answer: A lip tie is a restriction of the labial frenum, the band of tissue that connects the upper lip to the gum above the front teeth. It only matters clinically when it limits how the upper lip moves in a way that affects feeding, lip seal at rest, oral hygiene, or speech. A lip tie functional impact assessment exists to answer one question: is this tissue restricting function for this patient, or is it simply visible anatomy that nearly everyone has?
What a Lip Tie Actually Is, and What It Isn’t
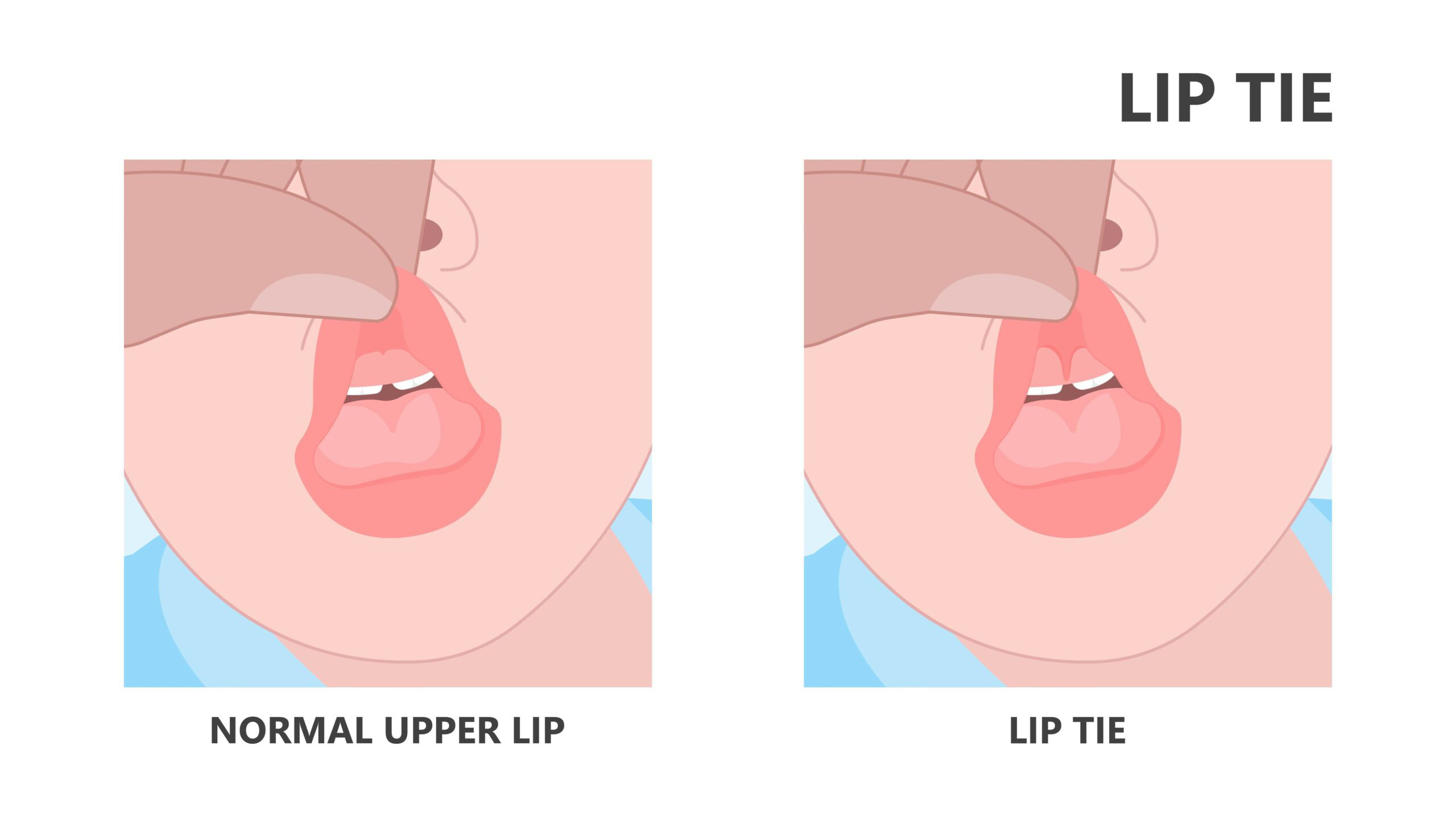
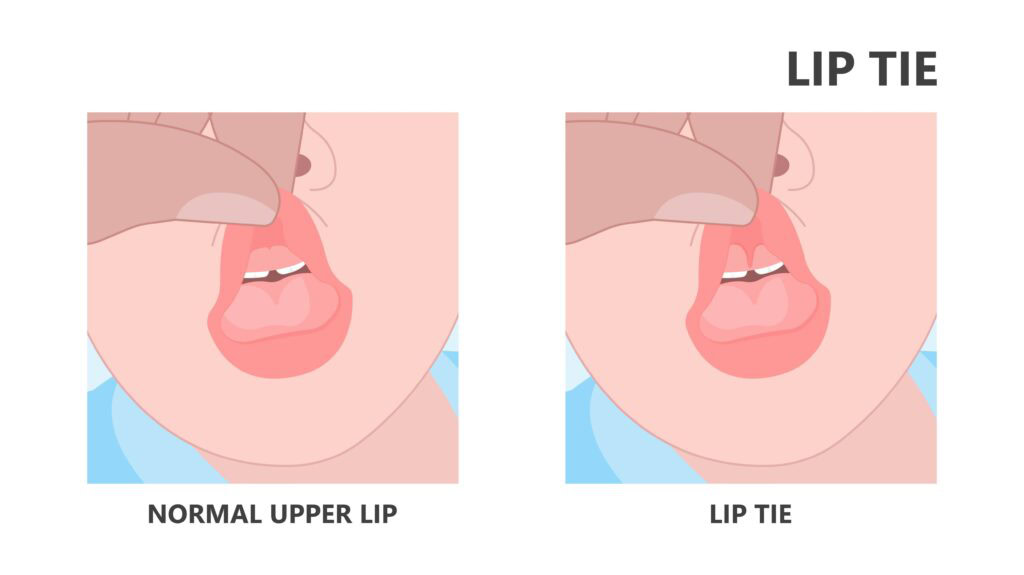
A lip tie is a restriction of the labial frenum, the small band of tissue that connects the upper lip to the gum tissue above the upper front teeth. When that tissue is short, thick, or attaches low on the gum, close to or between the upper front teeth, it can restrict how far the upper lip lifts, flanges outward, and moves on its own.
Here is the distinction that matters most, and it is the one that gets skipped: not every visible upper labial frenum is a functional problem. Almost everyone has a labial frenum, so the question is never whether tissue is present, because it usually is. The question is always whether that tissue is restricting function in a way that is clinically meaningful for the patient sitting in front of you.
When we start labeling every visible frenum a lip tie, and then treating every lip tie as something that automatically needs revision, the whole area gets muddy fast. The conversation has to stay anchored to function, not to anatomy alone.
The Functional Problems Linked to Restricted Upper Lip Mobility
When the upper lip cannot move freely, the effects tend to show up in a few predictable places. Here is where to look:
- Nursing and bottle feeding. A restricted upper lip cannot flange outward the way it needs to during latch. In breastfed infants, that often produces a shallow latch, a poor seal, air ingestion, clicking during feeding, and real nipple pain for mom. In bottle-fed infants, the same mechanical limitation shows up as seal breaks, more air intake, and faster fatigue.
- Oral hygiene. A lip tie that attaches between the upper front teeth can create a gap, or diastema, and makes it harder to clean the gum line in that spot. This is one of the main reasons pediatric dentists and dental hygienists flag lip ties, because the tissue forms a pocket that is tough to keep clean and more prone to decay.
- Speech precision. The bilabial sounds, meaning /p/, /b/, and /m/, all need the lips to come together fully. A restricted upper lip can affect how precisely a child produces them, though this is far less often the primary driver of a speech difficulty than tongue restriction is.
- Oral resting posture. A restricted upper lip may not settle into an easy, relaxed seal at rest. When closing the lips takes real muscular effort, kids tend to default to lips apart, and that opens the door to mouth breathing and the whole cascade of myofunctional consequences that follows it.
That last one deserves emphasis. Lip seal at rest is where a lip tie quietly drives a much bigger pattern, and it is the piece providers miss most often.
How a Lip Tie Functional Impact Assessment Differs From Tongue Tie Assessment
Tongue tie assessment centers on the lingual frenum: how restricted it is, how well the tongue elevates and moves, and what that means for swallow, speech, and breathing. A lip tie functional impact assessment asks a different set of questions, and it needs its own set of observations. [INTERNAL LINK: tongue tie assessment guide]
When you assess the lip, you are looking at:
- Where the frenum attaches relative to the gum line and the front teeth.
- Whether the lip blanches when you lift it, since gum tissue that turns white along the frenum points to a tight, restrictive attachment.
- How far the upper lip lifts and flanges outward through its full range.
- Whether there is a midline diastema sitting alongside a low frenum attachment.
- What the lip does at rest, which is often the most telling observation of all.
The blanch test is your simplest, most practical tool here. Gently lift the upper lip, and if the gum tissue blanches noticeably along the frenum, you are likely looking at a restrictive attachment. If the gum stays pink, the frenum has more give to it.
One more thing, and it is not optional: neither the lip nor the tongue assessment is complete without the other. Lingual and labial restrictions frequently travel together and interact, so assessing one in isolation leaves you with half a clinical picture, which is right back where this whole post started.
When the Lip Tie Is the Driver, and When Something Else Is Going On
This is the clinical judgment piece, and it is the part that good training actually builds in you over time.
A lip tie tends to be most functionally significant in infancy, when latch and feeding mechanics are the immediate concern. In older children and adults, a labial frenum can look prominent without being the main thing driving the presentation, because tongue posture, breathing pattern, or swallow dysfunction may be contributing far more to what you are seeing.
So the question to keep asking is twofold. First, if I address this, will the patient’s function meaningfully improve? Second, what else has to be addressed at the same time for that improvement to actually hold?
Here is the honest answer most people skip: a lip tie revision without myofunctional therapy to retrain rest posture, lip seal, and the broader pattern will rarely give you lasting results. The revision changes the structure, but function still has to be retrained, and that does not happen on its own.
Where Myofunctional Therapy Fits in Lip Tie Treatment
Myofunctional therapy earns its place in lip tie cases on both sides of a revision, and in plenty of cases where no revision is on the table at all.
- Before a revision, the work focuses on lip awareness, gentle mobilization within the lip’s current range of motion, and establishing nasal breathing.
- After a revision, you are rebuilding upper lip mobility and strength, retraining lip seal at rest, and addressing whatever other myofunctional contributors are in the picture.
- When revision is not indicated or not elected, myo therapy can still take on the compensatory patterns and improve lip posture, seal, and function within the anatomy the patient already has.
The structure is only ever half the work. Retraining the function is the other half, and it is the half that determines whether the result lasts.
A Simple Framework for Your Next Lip Tie Case
The next time a possible lip tie lands on your schedule, run it through these steps before anyone starts talking about revision:
- Confirm there is a true restriction, not just visible tissue. Use the blanch test and watch the lip’s full range, rather than judging by the look of the frenum alone.
- Map the functional impact. Check feeding, lip seal at rest, oral hygiene access, and speech, then decide which of these is actually affected for this patient.
- Assess the tongue in the same visit. Lingual and labial restrictions interact, so never evaluate one without the other.
- Ask whether the lip tie is really the driver. Especially past infancy, weigh tongue posture, breathing, and swallow before you assume the lip is the main contributor.
- Build the myo plan first. Whether or not a revision happens, function has to be retrained, so the therapy plan is what makes any structural change stick.
Run a lip tie functional impact assessment this way and you stop guessing. You will know whether you are looking at a clinically meaningful restriction or simply anatomy, and you will know what the patient needs next.
Ready to Make These Calls With Confidence?
If you want to assess and treat tongue and lip tie cases with this kind of clinical confidence, that is exactly what the Tongue Tie Bootcamp and The Myo Membership® are built to give you, which is the framework to make these calls and a community of clinicians to talk them through as the real cases land on your schedule.