If you’ve been in a feeding therapy room lately, ARFID vs pediatric feeding disorder has almost certainly come up. A parent mentions it. A pediatrician puts it in a referral note. A colleague asks if you “work with ARFID kids.”
And you probably nodded along while quietly wondering: wait, is that what I’m actually treating? Or is it something else?
Here’s the truth: the overlap between ARFID (Avoidant/Restrictive Food Intake Disorder) and Pediatric Feeding Disorder (PFD) is real, clinically significant, and genuinely confusing—even for experienced therapists. This post is going to clear it up.

What ARFID Actually Is (And Isn’t)
ARFID is a DSM-5 psychiatric diagnosis describing a persistent disturbance in eating or feeding that causes significant weight loss, nutritional deficiency, dependence on enteral feeding or oral supplements, or marked interference with psychosocial functioning.
What separates ARFID from ordinary picky eating is severity and functional impact. Children with ARFID aren’t going through a phase — their eating is restricted enough to affect growth, nutrition, or daily life, and that restriction isn’t explained by food unavailability, cultural practice, or an underlying medical condition.
ARFID has three recognized subtypes:
- Sensory sensitivity — avoiding foods based on texture, smell, or appearance
- Lack of interest in eating — low appetite, forgetting to eat, general disinterest in food
- Fear of aversive consequences — choking, vomiting, or allergic reaction, whether or not a prior incident has occurred
One important boundary: ARFID is a psychiatric diagnosis assigned by a psychologist or psychiatrist. As an SLP, OT, or PT, that determination is outside your scope.
What Pediatric Feeding Disorder Is
Pediatric Feeding Disorder (PFD) is a medical diagnosis, ICD-10 R63.31 (chronic) or R63.32 (acute), defined as impaired oral intake that is not age-appropriate, associated with medical, nutritional, feeding skill, and/or psychosocial dysfunction.
The PFD framework was developed to give the interdisciplinary feeding community a consistent shared language. It captures the full complexity of why a child isn’t eating: structural contributors, medical contributors, oral motor and sensory contributors, and the parent-child feeding relationship, all under one umbrella.
PFD is inherently an interdisciplinary diagnosis. It requires looking at the whole child across medical, nutritional, oral motor, and relational domains not a call any single clinician makes alone.
Key Differences Between ARFID and PFD
While ARFID and PFD can look similar on the surface, their underlying mechanisms and treatment approaches differ in important ways.
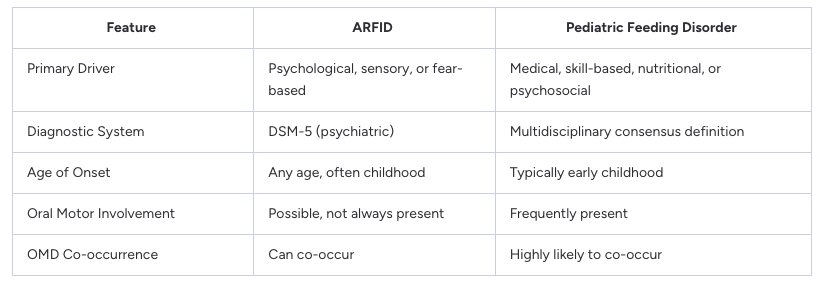
It is also worth noting that a child can meet criteria for both diagnoses simultaneously. The presence of one does not rule out the other.
Where They Overlap And Where Clinicians Get Confused
Here’s where it gets messy: a child can have both.
A child with ARFID who avoids foods due to sensory sensitivity may also have underlying oral motor dysfunction driving that texture aversion. A child with PFD rooted in medical trauma may develop fear-based restriction patterns that look exactly like ARFID.
A December 2024 consensus statement from the interdisciplinary feeding community identified 10 key points on the PFD-ARFID overlap, including that these diagnoses are not mutually exclusive and that treatment must address all contributing factors not just the psychiatric presentation.
The confusion typically runs in one of two directions: a clinician sees food restriction and jumps to ARFID without fully evaluating structural, oral motor, and medical contributors — or a team focuses on medical and skill-based pieces while missing the psychological and relational components entirely.
What Your Clinical Role Actually Is
As a feeding therapist, whether you’re an SLP, OT, or PT, your lane is the oral motor and sensory evaluation, the functional feeding assessment, and treatment directed at skill-based and sensory contributors.
You are not diagnosing ARFID. You are evaluating and treating within your scope.
What you can do:
- Screen for signs of ARFID-pattern presentation and document your findings clearly
- Communicate with the broader team to ensure the right referrals happen
- Flag when a child’s food restriction appears primarily driven by psychological factors outside your scope
- Advocate for interdisciplinary care
- Build a clinical reasoning framework that distinguishes what’s structural, sensory, behavioral, and relational — and know when each contributor needs its own team member
Your role isn’t diminished by those boundaries. It’s defined by them.
The ICD-10 Codes That Matter for Your Documentation
R63.31 — Pediatric feeding disorder, chronic
R63.32 — Pediatric feeding disorder, acute
F50.82 — Avoidant/Restrictive Food Intake Disorder
Knowing the distinction between these codes isn’t just for billing — it shapes how you communicate with referral sources, how you frame treatment plans, and how you position the interdisciplinary team around a complex case.
Why Your Training Foundation Matters More Than You Think
Navigating ARFID vs. PFD in a real clinical case requires more than reading a blog post. It requires the kind of clinical reasoning that helps you hold multiple hypotheses simultaneously, evaluate systematically rather than pattern-matching to the most recent term you heard, and communicate confidently with the broader team.
That clinical reasoning is built through structured, comprehensive training — the kind that takes you through development, assessment, oral motor function, sensory processing, and medical complexity all at once, not in isolated CEU hour chunks.
If you’re finding yourself uncertain in complex feeding cases, that’s not a character flaw. It’s a training gap. And it’s fixable.
Ready to build the clinical foundation that makes complex cases feel manageable? Learn more about Feed The Peds® at feedthepeds.com