An opinion piece was published in the ASHA Leader Live and it included many fallacies that need to be addressed. We do not always feel the need to correct mis-information, however, when it involves feeding, oral motor therapies, and tongue ties we want to ensure that parents and therapists are well informed on evidenced based practice.
Especially when it is published in the ASHA Leader Live, the certifying organization of Speech Language Pathologists & Audiologists.
It seems anyone can title a post or article “misinformation” and gain traction. We have NO desire to bring you anything but the truth. Your child’s health and optimal development are WHY we share! To put the power back in your {the parents/caeregivers} hands.
The following questions were asked and answered in the article “Clarifying Social-Media Misinformation About Pediatric Feeding Disorders”
We don’t dabble in “misinformation,” rather we back our work in facts and science.
[1] Do Sippy Cups cause speech, feeding, and airway issues?
What’s the big deal with sippy cups anyway? Sippy cups promote an immature oral motor pattern similar to the one used when drinking from a bottle called the suckling reflex. In this oral motor pattern, the tongue, lips, and jaw all work together when sucking. The muscles of the mouth should develop and work independently of each other as well as in harmony with one another.
Sippy cups do not encourage the muscles of the mouth to continue developing into more mature patterns needed for chewing, swallowing, speech and can encourage the tongue to sit in a low forward position in the oral cavity. Tongue position is a critical piece of proper oral motor development.
Our tongue is our natural palate expander, our lips are our natural braces.
When these muscles are functioning optimally, our palate should be wide enough to accommodate ALL of our teeth and our lips should be strong enough to aid in keeping our teeth straight. A sippy cup reinforces wrong tongue position and immature oral motor patterns.
If we encourage a immature oral motor pattern and a forward resting posture of the tongue with the use of a sippy cup, we may see a lisp and disrupted dental development. A sippy cup also holds the tongue down which makes elevating it for speech and feeding purposes more difficult. We need tongue tip elevation for production of speech sounds /t, d, n, l/ and proper swallowing.
Sippy cup use leads to: less mature swallow pattern ➡️ forward resting posture of the tongue or tongue thrust ➡️ open mouth posture at rest ➡️ speech sound development impacted due to tongue thrust ➡️ appetite cues reduced and dental development impacted
From a dental perspective, according to Dr. Mark Burhenne:
“Sippy cups prevent normal development of the mouth. Sucking from a sippy cup, bottle feeding and suckling a mother’s breast are not all equal. The motor activity of suckling a breast allows the child’s oral cavity to develop properly.
A nipple is soft and deforms when the child sucks on it — it takes a different shape inside the mouth of the child and helps promote proper development of all the oral structures, including jawbone, palate, teeth, and oral cavity. It has the child learn the proper motor function of the tongue.
Sucking on a rigid piece of plastic doesn’t allow for this and can actually misshape the oral cavity and result in problems later in life like speech, airway, sleep quality, and facial form and aesthetics.”
Read more at Ask the Dentist: https://askthedentist.com/sippy-cup-dangers/
References:
The development of oral motor control and language: https://pubmed.ncbi.nlm.nih.gov/17048804/
Why mouth breathing can be detrimental: https://link.springer.com/article/10.1007/s11325-015-1154-6
Sippy Cups 3 Reasons To Skip Them and What To Offer Instead: https://leader.pubs.asha.org/do/10.1044/sippy-cups-3-reasons-to-skip-them-and-what-to-offer-instead/full/
Transitioning To Cups from Breast/Bottle
Alberga, A. S., Pickett, W., & Jelalian, E. (2010). Sippy cups and childhood obesity: What is the evidence? Clinical Pediatrics, 49(8), 717-722.
Bishara, S. E., Laffoon, J. F., & Jakobsen, J. R. (2002). A longitudinal study of the effect of sucking habits on the dentition and orofacial structure of young children. American Journal of Orthodontics and Dentofacial Orthopedics, 121(4), 391-397.
Kumpulainen, S. (2012). The role of sippy cups in the development of oral posture. Journal of Orofacial Orthopedics, 73(1), 1-7.
Pereira, M. B. B., Pereira, V. B. P., Pereira, V. B. P., Pereira, V. G. F., Paula, V. M. B., Caetano, A. P. F., & Amaral, W. N. (2022). Randomized trial of a photography-aided behavioural intervention to reduce risk factors for caries and malocclusion in high-risk infants. International journal of dental hygiene, 20(3), 471–478. https://doi.org/10.1111/idh.12507
Sakuma, K. (2015). The effects of sippy cups on oral development. Pediatric Dentistry, 37(3), 222-228.
Shulman, J. (2015). The impact of sippy cups on speech and oral motor development. American Speech-Language-Hearing Association.
[2] Can oral motor exercises improve the skills needed to transition to solid, chewable foods?
Oral motor therapy is often the gateway to being able to safely manage foods for many children. When children come for feeding therapy and are unable to chew, and swallow food safely, we must first address the underlying deficit in the oral motor musculature to build up the strength, endurance, and motor planning skills needed to safely chew, move the food anterior-posterior in the oral cavity, and swallow safely.
These skills are addressed using oral motor therapy exercises which have been established over many years of evidenced based practice and research. If we give food to practice and learn these skills too soon, it could be detrimental to the child!
“ORAL MOTOR INTERVENTIONS SUPPORT PRE-FEEDING SKILLS BASED ON A TASK ANALYSIS OF THE UNDERLYING ORAL SENSORY MOTOR SKILLS REQUIRED FOR A SAFE AND EFFECTIVE NUTRITIVE FEEDING (OVERLAND & MERKEL-WALSH, 2013).” Robyn Merkel-Walsh MA, CCC-SLP, COM®
Evidence that oral motor interventions improve skills needed to transition to solid and chewable foods:
Pediatric Oral Sensorimotor Interventions for Chewing Dysfunction: A Scoping Review
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8585681/
The Effectiveness of Oral Sensorimotor Intervention in Children with Feeding Disorders
https://link.springer.com/article/10.1007/s40474-021-00236-y
Early oral-motor interventions for pediatric feeding problems: What, when and how
https://psycnet.apa.org/fulltext/2014-52008-004.html
Effect of oral motor facilitation technique on oral motor and feeding skills in children with cerebral palsy : a case study, Extracted from:
https://pubmed.ncbi.nlm.nih.gov/36324103/
Robyn Merkel-Walsh MA, CCC-SLP, COM®️ https://www.facebook.com/groups/296453726693
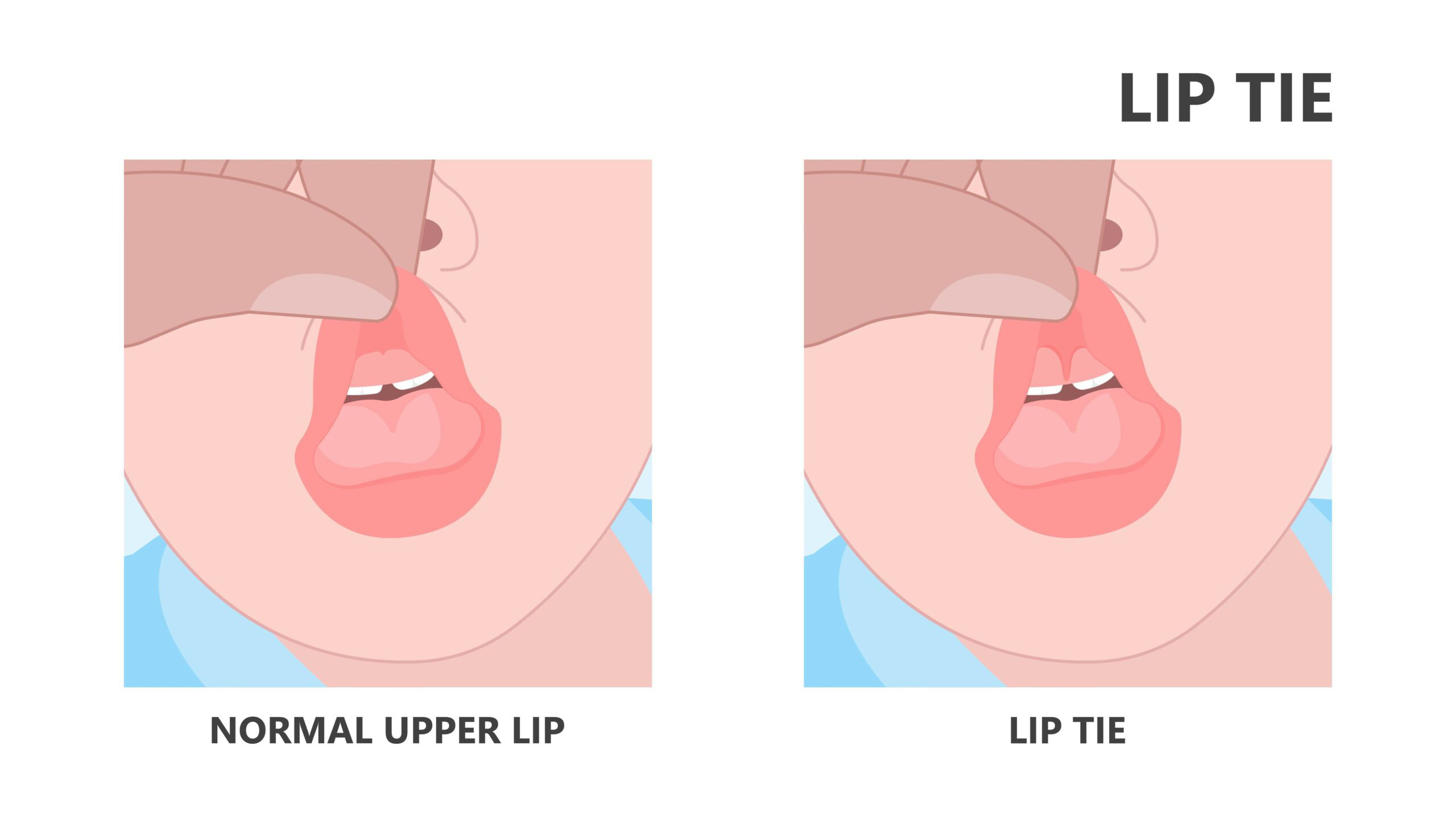
[3] Can ankyloglossia, or tongue tie, cause feeding or speech difficulties in children of any age?
The field of research supporting how tongue ties can negatively affect speech, language, and feeding is growing wildly. You have to ignore the evidence to say otherwise. Research comes from not only the field of speech pathology but other fields as well.
In practice, I have often seen children who made little to no progress on speech sounds and/or in feeding therapy until following a frenectomy (following optimal timing and preparation, of course). After the frenectomy, their skills blossomed like never before!
Below, we reference just a few of the many research articles outlining how tongue tie can affect feeding and speech and how a frenectomy aids in better function, increased speech, language, and feeding outcomes for some children.
Baxter, R., Merkel-Walsh, R., Baxter, B. S., Lashley, A., & Rendell, N. R. (2020). Functional improvements of speech, feeding, and sleep after lingual frenectomy tongue- tie release: A prospective cohort study. Clinical Pediatrics, 000992282092805.
Baxter, R., & Hughes, L. (2018). Speech and Feeding Improvements in Children After Posterior Tongue-Tie Release: A Case Series. International Journal Of Clinical Pediatrics, 7(3), 29-35.
Evidence that a frenectomy/tongue tie release aids in breast feeding: Ghaheri et al., 2021; Buryk et al., 2011), and preliminary evidence continues to evolve regarding speech and feeding beyond the breast (Baxter et al., 2020; Ghayoumi-Anaraki et al., 2022)
Effectiveness of Frenuloplasty in Ankyloglossia on Speech Quality: A Systematic Review, Extracted from: https://oamjms.eu/index.php/mjms/article/view/9604
[4] Do lip and buccal ties cause feeding and speech issues in infants and children?
The evidence to support that buccal and lip ties can lead to feeding and speech issues is emerging. Clinically, we see this very often in practice. We can speak to the hundreds and even thousands of infants and children who have come to our offices for services and have gained much improvement from releasing buccal and lip ties when nothing else had worked for them. We will always complete a thorough functional assessment before making any recommendations. Afterall, structure is only one piece of the puzzle.
Some research that supports buccal and lip ties causing feeding and speech issues in children:
Batista Borges Pereirs, M. (2022) Tongue-and lip-tie beyond breastfeeding difficulties. Jaw Functional Orthopedics and Craniofacial Growth. 2(2). DOI https://doi.org/10.21595/jfocg.2022.22790
Baxter, R, Merkel-Walsh, R, Lahey, L, Knutsen, C, Zaghi, S. The buccal frenum: Trends in diagnosis and indications for treatment of buccal-ties among 466 healthcare professionals. J Oral Rehabil. 2023; 00: 1-11. doi:10.1111/joor.13609
Ghaheri, B. A., Cole, M., Fausel, S. C., Chuop, M., & Mace, J. C. (2017). Breastfeeding improvement following tongue-tie and lip-tie release: A prospective cohort study. The Laryngoscope, 127(5), 1217–1223. doi:10.1002/lary.26306
These are just a few of the current literature to support that yes, in fact lip and buccal ties DO impact speech and feeding. Not to mention the countless reports from caregivers and parents who experience the dramatic improvement following releases of tip or buccal ties and report back.
[5] Is infant reflux normal?
While infant reflux is common in our culture, it is not normal. Common does not equal typical/normal!
Under the best circumstances, a baby should NOT experience reflux.
A small amount of spit up may occur with an infant, however, if it occurs often, in large amounts, and over a long period of time it can cause damage to the esophagus.
It’s important to seek out a professional to rule out if the infant might be swallowing air and actually refluxing milk, which can be linked to oral motor dysfunction and possibly oral ties. Food allergies may also be a culprit of excessive spit up/reflux and should be addressed right away, not ignored.
We should also take into consideration how much, how often, what the spit up looks like when determining if a babies spit up is within the “normal” realm or needs further assessment and remediation.
Evidence that infant reflux is not normal & tongue-tie procedures can improve outcomes:
Hill, R. R., & Pados, B. F. (2023). Gastrointestinal symptom improvement for infants following tongue-tie correction. Clinical Pediatrics, 62(2), 136–142. https://doi.org/10.1177/00099228221117459
Lechien J. R. (2023). Pediatric laryngopharyngeal reflux: an evidence-based review. Children (Basel, Switzerland), 10(3), 583. https://doi.org/10.3390/children10030583
Vandenplas, Y., Orsi, M., Benninga, M., Gatcheco, F., Rosen, R., & Thomson, M. (2023). Infant gastroesophageal reflux disease management consensus. Acta Paediatrica (Oslo, Norway: 1992), 10.1111/apa.17074. Advance online publication. https://doi.org/10.1111/apa.17074